
Long-Term Methadone Use: What Patients Wish They Knew From the Start
This information is for educational purposes only and is not intended to replace professional medical advice. It does…

Suboxone and methadone are two different medications that are both used to treat opioid use disorder.
Skip To
Similarities | Differences | Switching Medications | Get Medication | Ask a Question
No, but they share many similarities in treating the same condition, opioid use disorder.
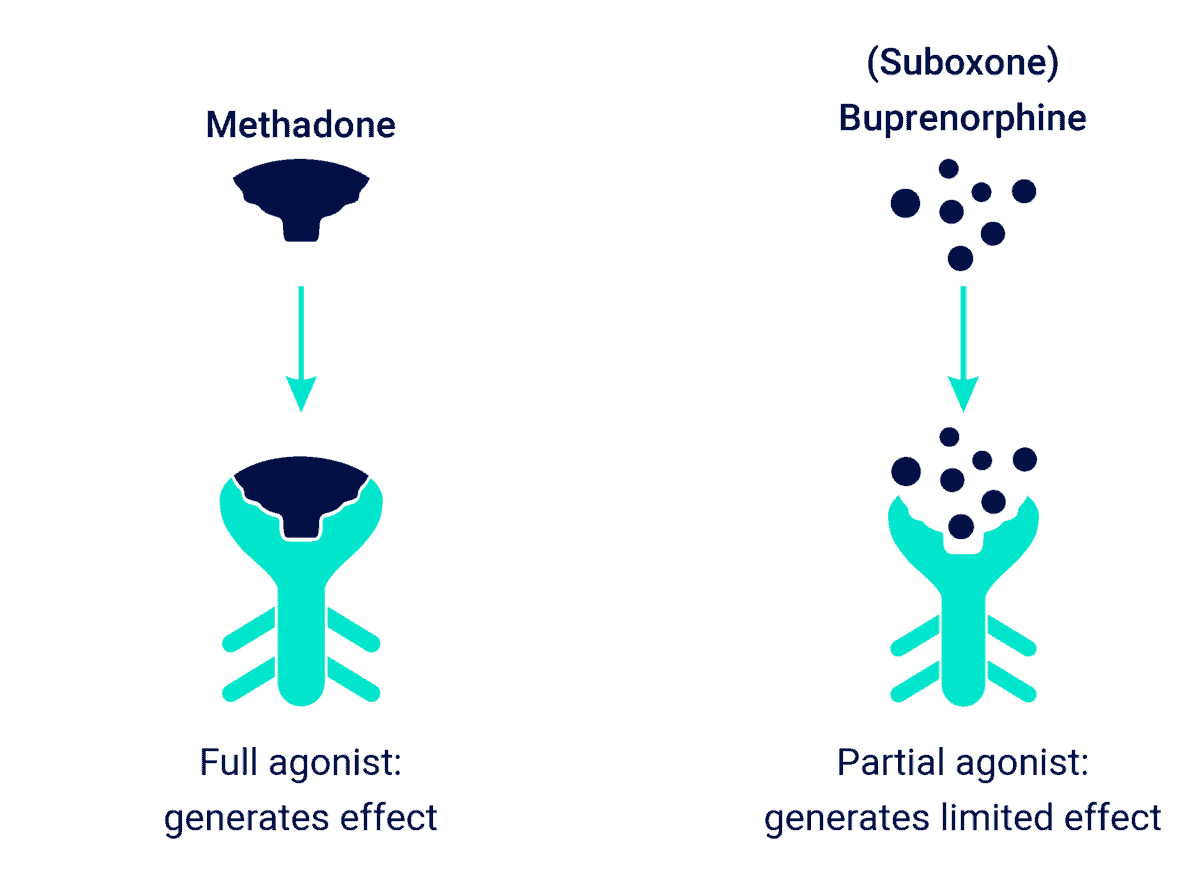
How Suboxone and Methadone Work in the Brain
Even though both help people with opioid use disorder, they are different medications.
| Medication | Methadone | Suboxone (Buprenorphine) |
| Mechanism | Full opioid (agonist) | Partial opioid (agonist) |
| Route of Administration | Oral (Dissolvable tablet, Pill, Liquid) | Film dissolved in mouth Oral Pill Injection in stomach (Subloclade) |
| Dosing | Daily | Daily for film / pill Monthly for injection |
| Available for Substance Use | Specialized Opioid Treatment Program (OTP) license | Doctors that apply for specialized certification |
Because it’s a full-agonist opioid, methadone is tightly regulated. Patients must report to a methadone clinic to get their dose dispensed to them. After several months of success, patients take home more methadone dosage over time and the requirement for check-ins end up similar to Suboxone eventually.ⓘ
See also: What is a Methadone Clinic?
Suboxone can be filled at the pharmacy like any other medication, but pharmacies too often refuse to provide Suboxone. A Suboxone clinic can dispense onsite.
See also: What is a Suboxone Clinic?
Suboxone is usually the first choice for opioid use disorder because people are less likely to abuse it and the naloxone blocker prevents overdose in case they do. However, methadone has been successfully treating opioid addiction for years and is a good option if you’ve already had success with it. Some switch to methadone if they haven’t been successful with Suboxone or want the extra daily accountability.
Do methadone and Suboxone have the same ingredients?
No, they are different medications with different ingredients.
Is methadone stronger than Suboxone? It could be said that methadone is stronger since the medication fully activates the opioid receptor while Suboxone only partially activates it. Though, both medications satisfy the brain’s craving for opioids.
What are the side effects of methadone vs. Suboxone?
Suboxone and methadone have similar side effects, including:
The biggest difference is that Suboxone doesn’t cause the feel-good, euphoric feelings of traditional opioids. It’s less intense than heroin or fentanyl, but you can get high off of methadone, which is why it’s given only at a clinic.
See also: Methadone Side Effects
Is methadone more effective than Suboxone?
Methadone and Suboxone are equally effective at treating opioid use disorder, though one study showed individuals on low doses of Suboxone (6 mg or less) are less likely to stay in treatment compared those taking methadone.ⓘ
No, you have to choose either Suboxone or methadone. Combining both medications is dangerous because both are opioids and because Suboxone contains naloxone, an opioid blocker.
This combination could cause an opioid / methadone overdose, but will more likely lead to severe precipitated withdrawal symptoms.
Combining Suboxone with methadone will not give you a high or relief, but will likely cause you to feel absolutely terrible including 10/10 body pain and vomiting.
See also: Drug Interactions with Methadone
If a patient is successfully treating their opioid addiction with methadone, there is no need to switch to Suboxone. But, if they continue to relapse or are non-compliant with the methadone program, Suboxone may be a better fit.
A patient’s methadone dose should be tapered down to 30mg before starting Suboxone and Suboxone shouldn’t be taken until at least 24 hours after the last dose of methadone.ⓘ Those on a low methadone dosage can usually transition without noticing an increase in symptoms or cravings. In one study, all 25 out of 25 participants transitioned successfully.ⓘ That said, withdrawals often lead to relapse, so the switch should be carefully coordinated by your doctor(s). See also: How To Get Off Methadone
It’s not as common to switch from Suboxone to methadone, but can be a good option when patient’s aren’t successful on Suboxone.
Switching from Suboxone to methadone is easier because methadone does not have an opioid blocker. Methadone should be started 24 hours after the last dose of Suboxone. The initial dose of methadone will be adjusted based on the patient’s last Suboxone dose.
See also: How to Get Off Suboxone
Symetria is a top-rated medication-assisted treatment (MAT) clinic, with locations throughout Chicago, as well as Fort Worth and Houston. All locations are in-network with insurances and offer both Suboxone and Methadone.
Get Methadone or Suboxone Here
Illinois Medication-Assisted Treatment
Texas Medication-Assisted Treatment
If you don’t happen to live in Illinois or Texas, try calling the number on the back of your insurance card. If you don’t have insurance, visit FindTreatment.gov and type in your zip code. Then, on the next page, use the free or slider scale filters.


Same-day appointments. Full insurance coverage. No judgment.
Fill out the confidential form and take your first step with Symetria today.
We respond within 1 business day. Your information is 100% confidential and HIPAA compliant.