
Suboxone® vs Methadone in Chicago: Which Is Right for You?
You aren’t looking for a textbook explanation when you’re exploring Suboxone® (buprenorphine-naloxone) versus methadone in Chicago. You’re looking…

Methadone overdose occurs when someone takes more than an appropriate amount of the medication or when a high dose is mixed with drugs like benzodiazepines or other opioids. Usually, methadone overdose is unintentional, caused by a lack of understanding of how methadone overdose works.
Skip To
Symptoms | Timing | Dose | Prevention | Treatment | FAQs | Ask a Question
Yes, methadone overdose is real and can be fatal. It’s an emergency situation that always requires 9-1-1 emergency intervention.
Methadone can cause slow or shallow breathing and dangerous changes in heartbeat that might be hard for the person to notice and react to before they become unconscious.
Methadone overdose symptoms get increasingly more concerning and can lead to death by respiratory depression if naloxone is not given to reverse the overdose.
See: Normal Side Effects of Methadone
On average, overdose symptoms start 3.2 hours after taking methadone.ⓘ
Death tends to occur 5-6 hours after taking methadone, regardless of whether the medication was taken orally or injected.ⓘ
All overdose symptoms should occur within 9 hours of taking methadone and subside within 24 hours.ⓘ Though there may be long-term damage that takes days or years to recover or is permanent.
The standard induction dose of methadone is only 20-30 mg even for patients with high tolerance to opioids. The dose is increased slowly usually to 80-120 mg for methadone maintenance.
The initial dose is only 10 mg for those with low or unknown opioid dependency. And, 50 mg is estimated to be a lethal dose for many people.ⓘ
See Also: The Methadone Dosage Article
The most obvious way to stay safe is getting methadone from a licensed physician, being honest with the provider about your drug usage and taking the medication as directed. Understanding the concepts below can also help.
The effects of methadone differ from other opioids. There is less of a “high” and it takes much longer to feel the full effects, usually peaking four hours later. Taking an extra dose of methadone within the first few hours to try to get to a “high” is a known cause of overdose.
Never use benzodiazepines (ie. Xanax) with methadone. Methadone and benzodiazepine both slow down the central nervous system. Combining these medications can cause airways to become too blocked to breathe.ⓘ
See also: Methadone Drug Interactions
Methadone cannot be injected safely. For anyone self-injecting whether by crushing methadone pills or tablets or even by injecting the syrup directly, please understand that this can cause serious or even life-threatening vein damage and increases the likelihood of methadone overdose.
Always keep naloxone (Narcan) on hand when using opioids. Naloxone can reverse a methadone overdose. You will not be able to administer naloxone yourself though, so be sure to have someone that can help when using any drug illicitly. Narcan can be obtained from a local methadone clinic, pharmacy or non-profit.
The best way to prevent a methadone overdose is to stop using the drug or any drugs illicitly. But, it’s never as easy as “just stopping.” If you live in Texas or Illinois, Symetria has outpatient clinics to help the withdrawal symptoms and mental chaos. (And, it’s covered by insurance).
Get Help with Methadone
Illinois Methadone Clinics
Texas Methadone Clinics
If this is an active overdose situation, please stop reading and call 9-1-1. Emergency services will walk you through the steps below.
The faster medical help is given, the less likely the overdose will be fatal.

Good Samaritan laws provide legal immunity from arrest and prosecution for drug possession when calling 9-1-1 in an overdose situation.
Kansas, Oklahoma and Wyoming are the only states without a specific law. In our home states, Texas passed the Jessica Sosa Act in 2021 and Illinois amended The Good Samaritan Act in 2012.
While the person who sold the drugs potentially could still face charges, the charge could be homicide if emergency services are not called and the victim dies.
It is always, always the right thing to call 9-1-1 in an overdose situation!
At the hospital, IV fluids, activated charcoal and laxatives may help flush methadone and any other drugs from the body a bit quicker.ⓘ A gastric lavage (ie. stomach pump) may also be performed.
Symptoms will also be treated, including a ventilator if breathing support is needed.
Vital signs including pulse, blood pressure and breathing rate will be constantly monitored.
Additional doses of naloxone are commonly required.
Many people survive opioid overdose without any long-term damage, but possible complications include:
The sooner medical care is provided, the less likely the person will face long-lasting effects.
As with any medication, the benefits of taking methadone should outweigh the risks, including overdose. Methadone can be a safe, life-changing medication for many patients.
(See also: Methadone Myths)
Methadone is a life-saving option for those that have not been successful on Suboxone or have been successful on methadone in the past.
Patients are monitored daily at the beginning and given appropriate amounts of medication that would not cause an overdose.
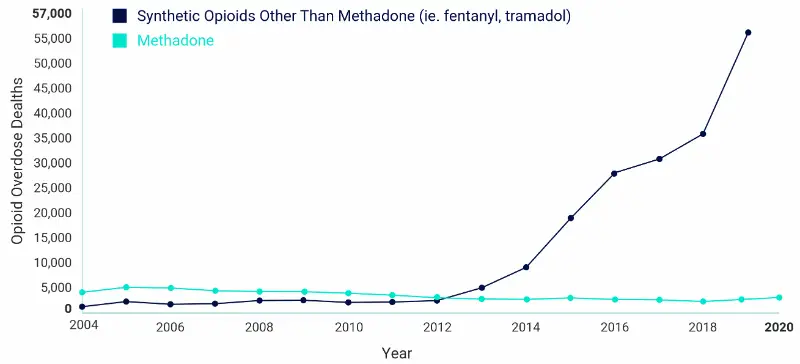
For most opioid use disorder patients, the risk of overdosing from not using methadone is much higher. Other opioids (ie. fentanyl / ISO) are 10x more likely to lead to overdose and death. The risk of a starting methadone treatment is always lower than illicit opioid use.
For chronic pain patients, methadone is not considered a first-choice medication and should not be used for mild pain, acute pain, “breakthrough” pain or on an as-needed basis. Methadone is appropriate if the pain is poorly controlled with other opioids or if the side effects of other medication options are too severe.ⓘ


Same-day appointments. Full insurance coverage. No judgment.
Fill out the confidential form and take your first step with Symetria today.
We respond within 1 business day. Your information is 100% confidential and HIPAA compliant.