
Suboxone® vs Methadone in Chicago: Which Is Right for You?
You aren’t looking for a textbook explanation when you’re exploring Suboxone® (buprenorphine-naloxone) versus methadone in Chicago. You’re looking…

Misinformation about methadone stops people from getting life-saving treatment. After you read, please help spread the facts about methadone.
In This Article
Methadone is a drug in the same way insulin or ACE inhibitors for heart conditions are drugs. We wouldn’t say someone taking other medications is addicted even though the medication is taken every day and required for the body to function correctly.
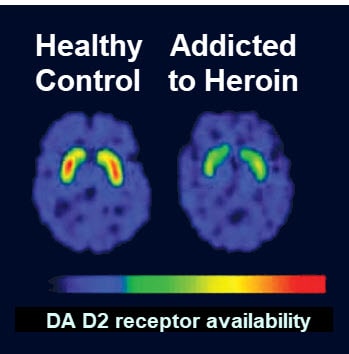
Some people find the comparison of methadone to drugs like insulin offensive because they see addiction as a choice. It’s not. Addiction is a chronic brain disease. And, just like many other diseases, medications (like methadone) can help.
Read more: Is Addiction a Choice?
Also, the myth that methadone is a substitute addiction implies that methadone is the same as prescription painkillers or heroin, which is scientifically inaccurate.
Methadone is designed to treat addiction and doesn’t activate opioid receptors in the same way as other opioid drugs. Overdosing from methadone (by abusing and mixing the medication) is 10x less likely than with other opioids.
Without getting too technical, methadone stabilizes brain chemistry to reduce cravings without giving off the same kind of euphoric feeling.
To learn more about how methadone works see: What is Methadone?
Those already abusing opioids would be unlikely to get a “high” from methadone — especially in a methadone clinic setting where doses are slowly increased over time.
Methadone is long-acting and doesn’t offer the intense, instantaneous “high” of short-term opioids like heroin or morphine.ⓘ
The misunderstanding of addiction as a disease fuels this myth. We need to change this stigma around addiction so more people feel comfortable seeking the treatment they need, which can include medications like methadone.
If you lined up people successfully on methadone maintenance with the general population, you would not be able to tell who is on methadone. Patients are able to function normally. In fact, some patients here go years without telling their parents or spouse about their treatment.
Ironically, this myth is most prevalent within the 12-step circles that should empathize most. “Like-me” bias instills judgment. (ie. I could find recovery without methadone, therefore everyone should find recovery without methadone).
However, research shows methadone is effective at stopping opioid abuse and more effective than 12-step programs. Studies from 1991, 2003 and 2007 show 70%+ methadone patients stop opioid misuse long-termⓘ, while 12-step success rate studies range from 10-50%.ⓘ
Read more: What Is The Success Rate Of Methadone?
Methadone can be used in opioid detox for just 3-10 days, but it can also be continued for years. There is not a specific time limit to use methadone that is right for every patient.
What is demonstrated consistently by researchers is that:
Because this data is unequivocal, the National Institute on Drug Abuse recommends methadone treatment be a minimum of 12 months.ⓘ
Patients actually have control over how often they need to come into a methadone clinic and how long their methadone treatment should last. After the first few weeks, patients can earn “take home” medication instead of going into the clinic. Eventually, patients may earn up to 28 days — coming to the clinic only monthly. And, it’s not “forever”.
When trying to stop cold turkey or within a matter of days, heroin may feel easier than methadone. However, the benefit of methadone is that it can be tapered down slowly to avoid most or even all withdrawal symptoms.ⓘ
See also: Getting Off Methadone
The discouragement of long-term methadone use is mostly seen on inpatient rehab websites. It could be because someone using outpatient methadone maintenance would not need inpatient rehab services. Though, hopefully, this is simply confirmation bias. (ie. Not seeking out or disregarding research which supports methadone use because of their singular belief in inpatient rehab).
Whether using methadone or not, those that struggle with opioid addiction are at higher risk of developing osteoporosis (ie. weak bones). This population has higher rates of tobacco use, HIV infections, poor diet and heavy alcohol use which are all known risk factors.
Research published by the Society for the Study of Addiction shows that methadone may contribute to mineral depletion of the bones specifically in lower-weight men with heavy alcohol use. There was no impact to bones found for women using methadone.ⓘ
Ultimately, methadone doesn’t “get in your bones” and asking your doctor about calcium and vitamin D supplements can help those at risk for osteoporosis.ⓘ
While there is a connection between general opioid abuse and osteoporosis, the myth of methadone getting into bones seems to stem from the bone aches of opioid withdrawal.
Methadone doses are increased slowly, so patients may experience manageable opioid withdrawal symptoms while starting methadone. (ie. Cold-turkey opioid withdrawal has been described as “feeling like every bone in my body was breaking.” With methadone, this may instead feel like “bone pain” that should be relieved with a dose increase).
Methadone is covered by every major health insurance company, though that doesn’t mean all methadone clinics accept all insurance. Each clinic decides which insurances to accept.
For example, many government-run methadone clinics focus on self-pay and Medicaid (ie. Family Guidance Methadone Clinic in Chicago). However, clinics like Symetria offer a usually much cheaper option for those with non-Medicaid insurance. (Methadone treatment here is in-network with nearly all private health insurance companies — Blue Cross Blue Shield, Aetna, Cigna / Evernorth, United Healthcare, Humana and many smaller plans — as well as Tricare and Medicare).
When patients are not aware that methadone is covered by insurance they take on the financial strain or delay seeking treatment altogether.
See also: Blue Cross Blue Shield Substance Abuse Coverage and United Healthcare Substance Abuse Coverage
Accepting insurance adds a layer of complexity that not all methadone clinics take on. (Even though using insurance lowers the overall cost for patients).
And, since most patients expect to self-pay for methadone, insurance companies sometimes make finding information about in-network methadone providers difficult.
If you live in Chicago, Dallas/Fort Worth or Houston, check your specific methadone insurance coverage below.
Ready to Start Methadone?
Illinois Methadone Clinics
Texas Methadone Clinics


Same-day appointments. Full insurance coverage. No judgment.
Fill out the confidential form and take your first step with Symetria today.
We respond within 1 business day. Your information is 100% confidential and HIPAA compliant.