

While taking opioids during pregnancy is dangerous, so is abruptly stopping opioid use. Physical withdrawals take a toll on the fetus and the risk of release is higher when pregnant.
For any patient that was taking opioids daily prior to getting pregnant, the American College of Obstetricians and Gynecologists recommends using buprenorphine or methadone the entire pregnancy.ⓘ
Skip To
Suboxone | Methadone | Cold-Turkey | Getting Help | Ask a Question
Can You Take Suboxone While Pregnant?
Buprenorphine (the main ingredient in Suboxone) is recommended for pregnant women that take daily opioids or Suboxone.
Pregnant patients already using Suboxone are usually advised to switch to buprenorphine-only medication for the remainder of their pregnancy (known as Subutex, though that brand is no longer manufactured).
Initial research showed that naloxone in Suboxone has a small risk of injury to the fetus. Though, more recent researchⓘ shows Suboxone is just as safe. Suboxone use during pregnancy will likely increase in the coming years, but for now, buprenorphine alone is the standard recommendation and has been proven safe in pregnancy.
Studies show no increase in anomalies of babies born to mothers using buprenorphine compared to the general population.ⓘ
Quitting Suboxone while Pregnant
It is not recommended to quit buprenorphine treatment during pregnancy.
Most women immediately look into <aWhitney, M. J., & Burke, T. F. (2012). Buprenorphine and pregnancy: A review of the evidence for safety and efficacy. *Journal of Addiction Medicine*, 6(5), 401-410.
Most women immediately look into how to get off Suboxone when they find out they're pregnant, but this desire is driven by social stigma and not the factual well-being of the baby. The research is clear that both mother and baby are better off on buprenorphine.
Suboxone When Breastfeeding
Breastfeeding is encouraged for women stable on anti-craving medications like Suboxone or methadone. Breastfeeding has been shown to decrease illnesses in babies, improve their nutrition and even reduce illness in the mother too.ⓘ
However, in the case of relapse or other opioid use, formula is a safer choice and breastfeeding should be stopped.
Suboxone & Pregnancy FAQs
Do they test for Suboxone when pregnant?
Women are not always tested for Suboxone while pregnant. Suboxone is not included on standard drug screens. It is also safe to use during pregnancy.
However, Suboxone (buprenorphine) is tested for during a newborn toxicology. Positive results are required to be reported to the state by the hospital. If the mother does not have a legal prescription for the Suboxone, it can lead to further investigation and actions from child welfare.
Read more: Drug Test For Newborns
Does taking Suboxone make it hard to get pregnant?
No, Suboxone does not affect fertility. The medication has no impact on a woman’s ability to get pregnant or a man’s ability to get someone else pregnant.
Can Suboxone cause a false positive pregnancy test?
No. A study of 27,001 patients showed no report of false positive pregnancy tests for those who take Suboxone.ⓘ
But, other mental health medications like methadone, diazepam (Valium), alprazolam (Xanax) or antipsychotics like clozapine or chlorpromazine have been linked to false positive pregnancy tests. It could also happen with a faulty test or because of timing. It’s recommended to wait one week after the expected period to take the test.ⓘ
Does Suboxone cause neonatal abstinence syndrome?
Buprenorphine can cause Neonatal Abstinence Syndrome (NAS). However, this condition is treatable and usually slightly less severe than using methadone.
Studies show no increase in anomalies of babies born to mothers using buprenorphine compared to the general population.ⓘ
Is Vivitrol safer than Suboxone while pregnant?
Naltrexone (Vivitrol) does not currently have enough data to support continued use during pregnancy. Though, the limited case studies that have been published show normal birth outcomes.
Until more research is conducted (especially on fetal effects), starting naltrexone would not be recommended for pregnant women.
The decision on whether to continue use for women already using naltrexone would weigh the lack of substantial safety data with the potential for relapse and known harm of opioid use during pregnancy.
Can You Take Methadone While Pregnant?
Not only is the medication safe, but methadone use during pregnancy is actually recommended by major health organizations — including the American College of Obstetricians and Gynecologists.
Pregnant women using methadone are more likely to get prenatal care and deliver at a hospital which dramatically improves outcomes for both mother and baby. ⓘ
Methadone also stabilizes the fetus and optimizes fetal growth after opioid addiction - including normalizing the intrauterine milieu, which is linked to cardiovascular issues.ⓘ
Read other: Methadone Myths
Methadone vs Buprenorphine in Pregnancy
While both methadone and buprenorphine are safe and recommended for opioid-using women during pregnancy, some studies lean toward buprenorphine as a better first-choice option.ⓘ
Buprenorphine has fewer drug interactions, dosing throughout pregnancy is more stable and any neonatal abstinence syndrome symptoms tend to be less severe.
However, methadone has more long-term data on infant and child effects and does not carry the risk of While taking opioids during pregnancy is dangerous, so is abruptly stopping opioid use. Physical withdrawals take a toll on the fetus and the risk of release is higher when pregnant.
For any patient that was taking opioids daily prior to getting pregnant, the American College of Obstetricians and Gynecologists recommends using buprenorphine or methadone the entire pregnancy.ⓘ
Skip To
Suboxone | Methadone | Cold-Turkey | Getting Help | Ask a Question
Can You Take Suboxone While Pregnant?
Buprenorphine (the main ingredient in Suboxone) is recommended for pregnant women that take daily opioids or Suboxone.
Pregnant patients already using Suboxone are usually advised to switch to buprenorphine-only medication for the remainder of their pregnancy (known as Subutex, though that brand is no longer manufactured).
Initial research showed that naloxone in Suboxone has a small risk of injury to the fetus. Though, more recent researchⓘ shows Suboxone is just as safe. Suboxone use during pregnancy will likely increase in the coming years, but for now, buprenorphine alone is the standard recommendation and has been proven safe in pregnancy.
Studies show no increase in anomalies of babies born to mothers using buprenorphine compared to the general population.ⓘ
Quitting Suboxone while Pregnant
It is not recommended to quit buprenorphine treatment during pregnancy.
Most women immediately look into how to get off Suboxone when they find out their pregnant, but this desire is driven by social stigma and not the factual well-being of the baby. The research is clear that both mother and baby are better off on buprenorphine.
Suboxone When Breastfeeding
Breastfeeding is encouraged for women stable on anti-craving medications like Suboxone or methadone. Breastfeeding has been shown to decrease illnesses in babies, improve their nutrition and even reduce illness in the mother too.ⓘ
However, in the case of relapse or other opioid use, formula is a safer choice and breastfeeding should be stopped.
Suboxone & Pregnancy FAQs
Do they test for Suboxone when pregnant?
Women are not always tested for Suboxone while pregnant. Suboxone is not included on standard drug screens. It is also safe to use during pregnancy.
However, Suboxone (buprenorphine) is tested for during a newborn toxicology. Positive results are required to be reported to the state by the hospital. If the mother does not have a legal prescription for the Suboxone, it can lead to further investigation and actions from child welfare.
Read more: Drug Test For Newborns
Does taking Suboxone make it hard to get pregnant?
No, Suboxone does not affect fertility. The medication has no impact on a woman’s ability to get pregnant or a man’s ability to get someone else pregnant.
Can Suboxone cause a false positive pregnancy test?
No. A study of 27,001 patients showed no report of false positive pregnancy tests for those who take Suboxone.ⓘ
But, other mental health medications like methadone, diazepam (Valium), alprazolam (Xanax) or antipsychotics like clozapine or chlorpromazine have been linked to false positive pregnancy tests. It could also happen with a faulty test or because of timing. It’s recommended to wait one week after the expected period to take the test.ⓘ
Does Suboxone cause neonatal abstinence syndrome?
Buprenorphine can cause Neonatal Abstinence Syndrome (NAS). However, this condition is treatable and usually slightly less severe than using methadone.
Studies show no increase in anomalies of babies born to mothers using buprenorphine compared to the general population.ⓘ
Is Vivitrol safer than Suboxone while pregnant?
Naltrexone (Vivitrol) does not currently have enough data to support continued use during pregnancy. Though, the limited case studies that have been published show normal birth outcomes.
Until more research is conducted (especially on fetal effects), starting naltrexone would not be recommended for pregnant women.
The decision on whether to continue use for women already using naltrexone would weigh the lack of substantial safety data with the potential for relapse and known harm of opioid use during pregnancy.
Can You Take Methadone While Pregnant?
Not only is the medication safe, but methadone use during pregnancy is actually recommended by major health organizations — including the American College of Obstetricians and Gynecologists.
Pregnant women using methadone are more likely to get prenatal care and deliver at a hospital which dramatically improves outcomes for both mother and baby. ⓘ
Methadone also stabilizes the fetus and optimizes fetal growth after opioid addiction - including normalizing the intrauterine milieu, which is linked to cardiovascular issues.ⓘ
Read other: Methadone Myths
Methadone vs Buprenorphine in Pregnancy
While both methadone and buprenorphine are safe and recommended for opioid-using women during pregnancy, some studies lean toward buprenorphine as a better first-choice option.ⓘ
Buprenorphine has fewer drug interactions, dosing throughout pregnancy is more stable and any neonatal abstinence syndrome symptoms tend to be less severe.
However, methadone has more long-term data on infant and child effects and does not carry the risk of precipitated withdrawal when starting the medication.
Methadone is usually the ideal choice for those who are:
- Not successful / compliant on buprenorphine
- Buprenorphine allergy
- Already successful on methadone or were successful on methadone in the past
A 2015 review of multiple studies show no difference between the medications on fetal death or anomalies, so the important question is which medication is more effective for the patient.ⓘ
Read more: Methadone vs Suboxone
Methadone Dosing While Pregnant
Women using methadone during pregnancy may require increased or split dosing — especially in the third trimester. (Split dosing means taking around the same amount of methadone, but taking it twice per day instead of once).
Don't be afraid to change your dose. Several studies show that an increase in dosage does not impact the likelihood, severity or duration of neonatal abstinence syndrome (NAS). And, split dosing actually showed lower rates of NAS.ⓘ
Read more: Methadone Dosage
Methadone Effects on Fetus
Methadone has been used since the 1970s and its impact on pregnant women and baby outcomes has been well-studied.
The data shows no increase in anomalies of babies born to mothers using methadone compared to the general population.ⓘ
While methadone may temporarily slow fetal heart rate and movement (usually around four hours after dosing), this is not known to cause harm to the fetus.ⓘ
Compared to untreated pregnant women, babies born to mothers using methadone were less likely to be premature and less likely to develop Neonatal abstinence syndrome (NAS). (If NAS does occur in newborns of methadone-treated mothers, it is usually less severe and breastfeeding has been shown to help).
Stopping Opioids "Cold-Turkey" During Pregnancy
Stopping opioid use while pregnant without the help of medications and the oversight of a doctor is extremely dangerous. The risk of relapse when detoxing while pregnant is as high as 90% and the severe withdrawal symptoms impact the fetus too. ⓘ
Relapse is always hard to resist when detoxing, but is nearly impossible with the chemical, physical and emotional changes of pregnancy. Any continued opioid use after a relapse can be avoided by instead seeking help. Additionally, overdoses are most common after a detox attempt.
Withdrawal symptoms can also be worse because the pregnancy already takes a toll on your body. If you are not able to eat or sleep and are feeling intense anxiety, your baby is impacted by that distress. And, your baby will go through their own withdrawals as well.
Going to an addiction clinic or rehab means less sickness and more long-term success.
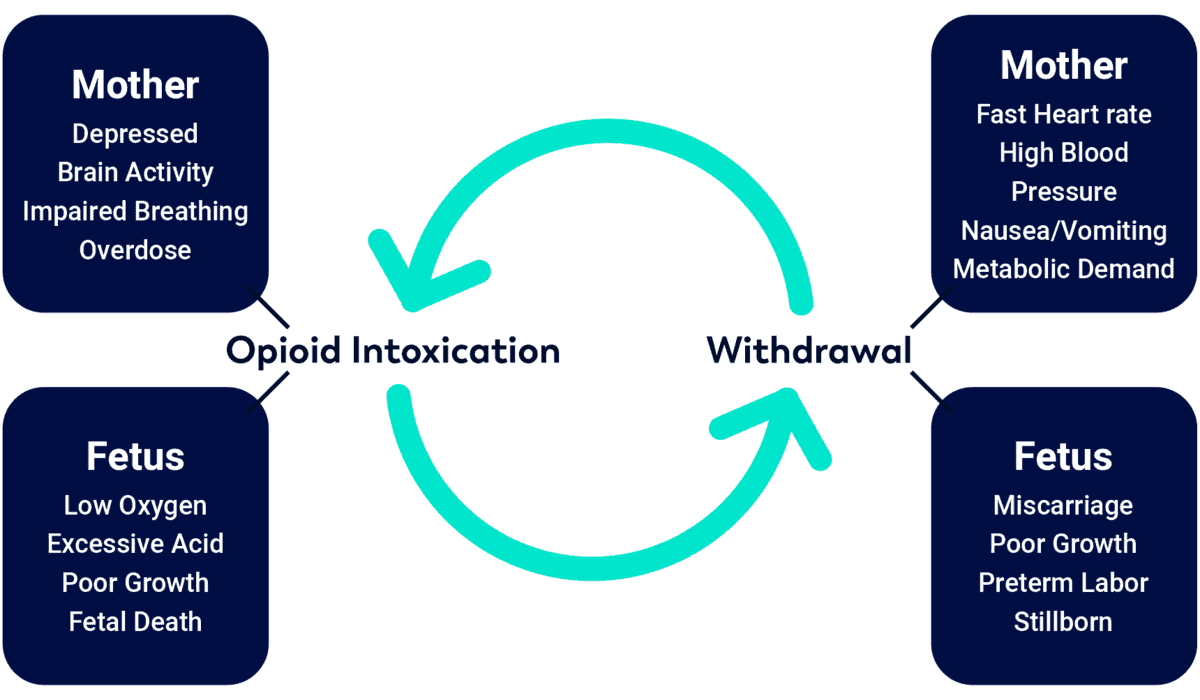
Effects of Opioid Use & Withdrawal on Mother and Fetus
Pregnancy & Opioids FAQs
Trying to quit on your own is more likely to lead to continued illicit opioid use than it is to lead to an ideal pregnancy.
What happens when using opioids while pregnant?
Chronic opioid use during pregnancy is dangerous for both mother and baby, linked to:
- Maternal death gauge
- Pregnancy complications: including placental abruption and preeclampsia
- Poor fetal growth
- Premature births
- Neonatal Abstinence Syndrome (NAS): newborn withdrawal symptoms
- Miscarriage or stillbirths
- Birth defects: including heart defects, gastroschisis, glaucoma and issues like spina bifida
If you used opioids while pregnant, the feelings of worry and guilt can be extremely harmful. Most babies, even those born with NAS, live a healthy and normal life, especially if illicit opioid use is replaced with buprenorphine or methadone.
Focus on treatment and giving you and your baby a dramatically better life.
Can taking opioids during pregnancy cause autism?
No, opioid use before or during pregnancy is not linked to an autism spectrum disorder diagnosis. Neither is opioid use while breastfeeding nor the father’s opioid use.
Can taking opioids when pregnant cause ear infections in infants?
Yes, babies and toddlers of mothers that took opioids while pregnant have significantly higher rates of ear infection (otitis media).ⓘ
Can pregnant women get opioids?
No, opioids are known to be dangerous during pregnancy for both mother and baby. A doctor wouldn’t prescribe opioids to a pregnant woman and would switch chronic pain patients to buprenorphine or methadone.
Can taking opioids keep you from becoming pregnant?
Some studies link opioids to lower fertility rates in women and men, but more than 20,000 babies are born in the U.S. every year dependent on opioids.
Male or female opioid use will not stop a woman from getting pregnant and in no way replaces birth control! However, if seeking fertility treatment, opioid use should be disclosed.
Getting Help for Opioids While Pregnant
Not all addiction treatment programs are able to accept pregnant patients, but women have both outpatient and inpatient options for care — including Symetria Recovery.
Even if you've used opioids while pregnant already, getting professional medical help now can prevent negative impacts on the pregnancy or involvement from social services. There is no shame in getting help!
Get Help for Opioids While Pregnant in Illinois or Texas
Illinois Outpatient Addiction Clinics
- Drug Rehab Chicago
- Drug Rehab Naperville
- Drug Rehab Joliet
- Drug Rehab Des Plaines
- Drug Rehab Palos Heights
- Drug Rehab Vernon Hills
Texas Outpatient Addiction Clinics